Yellow fever is back.
On May fifth, the World Health Organization issued an alarming yellow fever “situation report.” In it, the WHO said that a yellow fever outbreak was detected in Angola late in December 2015 and confirmed by the Institut Pasteur Dakar on 20 January 2016. This confirmation was followed by an increase in cases; as of 4 May 2016, Angola has reported 2149 suspected cases of yellow fever.
In addition to the cases found in Angola, three countries have now reported confirmed yellow fever cases exported from Angola: Democratic Republic of the Congo (37 cases), Kenya (two cases) and China (11 cases). Namibia has also reported a suspect yellow fever case exported from Angola. Exported cases are thought to have been infected in Angola but diagnosed in other countries.
In addition to Angola’s exported cases, a separate outbreak of yellow fever has occurred in Uganda. As of 4 May, 41 suspect cases of yellow fever cases have been reported in seven districts. According to available information, the clusters of yellow fever in Uganda are not linked to each other, or to the Angola outbreak. The sequencing results indicate high similarities with the virus which has caused Uganda’s yellow fever outbreak in 2010, which would imply that the virus has been living in animal reservoirs and then returned to human infection. A few cases of yellow fever also appear to have broken out in DRC separately from their Angola-exported cases.

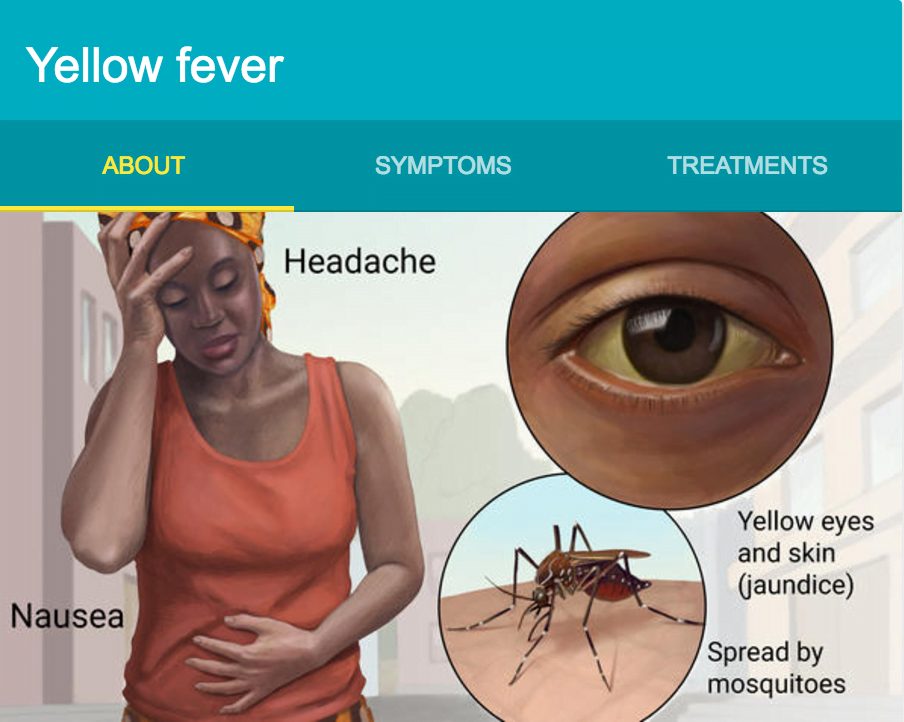
Yellow fever is a tropical viral disease with a painful history.
It was one of the most deadly diseases of the 19th century, killing large numbers of people on three continents – Africa and North and South America. Its spread was finally halted in the 1920s, when an effective vaccine was developed and widely distributed. The virus still causes 200,000 infections and 30,000 deaths every year globally, with nearly 90% of these occurring in Africa. If vaccination rates decline, the risk of resurgence increases.
The current outbreak is a complex and challenging situation. It can be looked at in two different ways.
The optimistic view suggests that the international health structures are doing their jobs. Surveillance tracked the virus early on, and the outbreak was contained before it could spread to many countries. Now that the outbreaks have been identified, targeted vaccination campaigns and better mosquito control can eliminate the virus.
The negative view suggests that yellow fever could follow the path of Ebola, or malaria. It is mosquito-spread, just like malaria and dengue fever. It can be hard to diagnose, and we have now seen that people can fly as far as China when already infected with the disease. Countries that have already failed at vaccination are unlikely to manage an effective emergency campaign. Yellow fever could just keep spreading through the same porous borders exploited by Ebola.
No matter which explanation proves most accurate, there are two main forces driving this upsurge. One driver is systemic.This outbreak is clear evidence of unvaccinated people – a symptom of weak health systems and governments that don’t prioritize health. There is a vaccine for yellow fever, so this kind of outbreak should not be happening. The second driver is human settlement patterns; yellow fever is often spread by monkeys. As human settlements encroach more and more on animal habits, zoonotic diseases like yellow fever are going to increase. This is basic epidemiology.
Because of the under-funding we’ve seen for so long, and the increased health burden caused by zoonotic diseases, ending the long-term risk of diseases like yellow fever – and Ebola, and malaria – will require major investment into better health systems throughout Africa. This outbreak is just the most recent reminder.